Phase4 (12~16weeks)
|
Goal |
Exercise |
|
◈ complete tendon healing mature repaired rotator cuff tissue
◈ advanced strengthening
◈ maximum tensile endurance
|
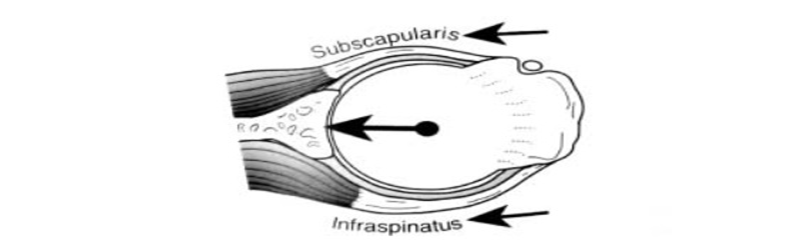
1. OKC strengthening * standing ER - infraspinatus & teres minor - standing AB90,ER - supraspinatus(at least after 16wks) - scaption(at least after 16wks), (at least after 24wks: large & massive tear) - Emphasize eccentric exercise
2. scapulo-thoracic exe * standing punch plus( SA activation):90~120° (after 16wks) - puch-up plus (wall ->table ->floor)
3. proprioception * rhythmic stabilization exe- F90°("statue of liberty position"), ABER position 4. plyometric exe overhead motion : throw against a wall, rebounder, weighted ball |
⇒ Remodeling repair tissue does not reach maximal tensile strength for a minimum of 12~16 weeks post repair
⇒ returned to maximal failure loads after only 26weeks of healing
⇒ Plyometric exe: only large & massive tear(at least 24weeks)


Postperative months 3~6
* No heavy overhead lifting and no acceleration of arm in sport.
* For massive tears and revision repairs, delay strengthening until 4 months postoperatively
Remodeling repair tissue does not reach maximal tensile strenght for a minimum of 12~16 weeks post repair.
Progressive post cuff strengthening
□ Progressive strengthening of the posterior cuff
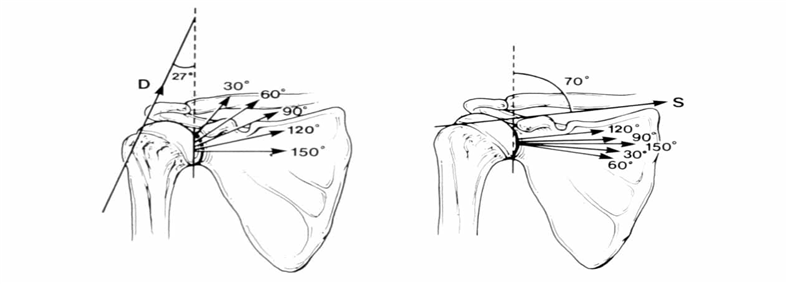
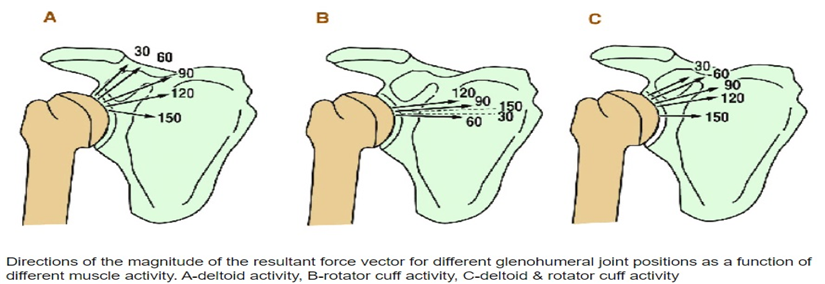
* performing external rotation of the shoulder at 30~45° degrees of abduction utilizing elastic resistance
□ high levels of infraspinatus and teres minor activation at 90° of abduction
* performing external rotation exercise, supraspinatus muscle activity is optimally generated
abduction
* performing external rotation exercise, supraspinatus muscle activity is optimally generated
Progressive OKC exe

Progressive CKC
□ Additionally, the push-up with a plus progresstion is a more advanced exercise that strengthens the serratus anterior muscle

Reference
Myers, Joseph B. shoulder muscle reflex latencies under various levels of muscle contraction. Clinical Orthopaedics & Related Research. 407:92-101, February 2003.
Musculoskeletal evidence based treatment
Frederick A. Matsen, III, Caroline Chebli and Steven Lippitt. Principles for the Evaluation and Management of Shoulder Instability. J Bone Joint Surg Am. 2006;88:647-659.
Morrey BF, An KN (1990) Biomechanics of the shoulder. In: Rockwood CR, Matsen FA (ed) The shoulder. Saunders, Philadelphia, pp 208–245Google Scholar.
Philip Mcclure, Lori A. Michener. Direct 3-dimensional measurement of scapular kinematics during dynamic movements in vivo. Published in Journal of shoulder and elbow surgery 2001
Parsons IM1, Apreleva M, Fu FH, Woo SL. The effect of rotator cuff tears on reaction forces at the glenohumeral joint. J Orthop Res. 2002 May;20(3):439-46.
Young Jin Jo1, Young Kyun Kim. Consideration of Shoulder Injury Prevention and Rehabilitation Exercise for Overhead Sports Population. Asian J Kinesiol 2019; 21(2): 40-50 · DOI: https://doi.org/10.15758/ajk.2019.21.2.40
Ofer Levy, Hannan Mullett, The role of anterior deltoid reeducation in patients with massive irreparable degenerative rotator cuff tears. Medicine Published in Journal of shoulder and elbow surgery2005 DOI:10.1016/j.jse.2008.04.005
https://www.hep2go.com/index_b.php?userRef=120148
Olivier A. van der Meijden, MD1. Rehabilitation after arthroscopic rotator cuff repair: Current concepts review and evidence-based guidelines. International Journal of Sports Physical Therapy · April 2012
'물리치료 공부' 카테고리의 다른 글
| Core (0) | 2020.10.18 |
|---|---|
| 척추전방전위증(Spondylolisthesis) (0) | 2020.10.04 |
| 어깨(회전근개) 수술후 재활 part 6(Rotator cuff tear repair Protocol Phase3 (8~12weeks)) (0) | 2020.09.06 |
| 어깨(회전근개) 수술후 재활 part 6(Rotator cuff tear repair Protocol Phase2 (4~8weeks)) (0) | 2020.08.30 |
| 어깨(회전근개) 수술후 재활 part 6(Rotator cuff tear repair Protocol Phase1 (1~4weeks)) (0) | 2020.08.30 |