요즘 어깨 통증으로 오시는 분들중에 이 증후군이 있으신 분들이 많습니다. 어깨 문제로는 흔히 라운드 숄더다 오십견이다.거북목이다. 회전근개 문제다.~ 이런말이 많지만 이러한 문제를 가지고 계신분들을 임상에서 보게 되면 견갑상신경이 포착되어있는 경우가 많습니다. 신경은 신체에서 아주 중요한 요소로 신경과 혈액순환이 원활하지 않으면 그 부분은 뭉치고 퍽퍽해지고 허혈이되어 힘이 떨어지고 통증을 유발합니다. ㅠㅠ 자 상세히 알아봅시다~!
견갑상신경– 경추5번6번 신경에서 분지되어 견갑상절흔을 통과하여 상견갑와로 들어가며 이후에는 극관절와 인대를 통과하여 아래로 주행, 극상근과 극하근을 지배하며, 어깨관절과 인대의 전체적인 감각에도 관여하는 신경입니다. 이 신경이
압박되면 어깨통증과 극상근 극하근 근력저하가 나타납니다.
원인
외상과 반복적으로 어깨를 부딪히는 운동이나 팔을 내전, 내회전을 많이하는 운동이 원인이 될 수 있으며
넘어지거나, 무거운 가방을 메고 다니는 경우 또한 위에서 말한라운드숄더 체형(견갑골이 앞으로 말린 경우)
선천적으로 견갑상절흔이 좁은 경우 이러한 증상이 나타날 수 있습니다.
증상
어깨 통증이 있으며 전체적으로 시큰하며어깨 뒤편에 깊은통증을 느낍니다.
외전 외회전 동작에서 힘이 떨어지며 근력약화가 장기간 지속되면 회전근개인 극상근 극하근이 위축될 수 있습니다.
□ Additionally, the push-up with a plus progresstion is a more advanced exercise that strengthens the serratus anterior muscle
Reference
Myers, Joseph B.shoulder muscle reflex latencies under various levels of muscle contraction.Clinical Orthopaedics & Related Research. 407:92-101, February 2003.
Musculoskeletal evidence based treatment
Frederick A. Matsen, III, Caroline Chebli and Steven Lippitt. Principles for the Evaluation and Management of Shoulder Instability.J Bone Joint Surg Am. 2006;88:647-659.
Morrey BF, An KN (1990) Biomechanics of the shoulder. In: Rockwood CR, Matsen FA (ed) The shoulder. Saunders, Philadelphia, pp 208–245Google Scholar.
Philip Mcclure, Lori A. Michener. Direct 3-dimensional measurement of scapular kinematics during dynamic movements in vivo.Published in Journal of shoulder and elbow surgery 2001
Parsons IM1, Apreleva M, Fu FH, Woo SL. The effect of rotator cuff tears on reaction forces at the glenohumeral joint.J Orthop Res. 2002 May;20(3):439-46.
Young Jin Jo1, Young Kyun Kim. Consideration of Shoulder Injury Prevention and Rehabilitation Exercise for Overhead Sports Population.Asian J Kinesiol 2019; 21(2): 40-50 · DOI: https://doi.org/10.15758/ajk.2019.21.2.40
Ofer Levy, Hannan Mullett, The role of anterior deltoid reeducation in patients with massive irreparable degenerative rotator cuff tears.Medicine Published in Journal of shoulder and elbow surgery2005 DOI:10.1016/j.jse.2008.04.005
Olivier A. van der Meijden, MD1. Rehabilitation after arthroscopic rotator cuff repair: Current concepts review and evidence-based guidelines.International Journal of Sports Physical Therapy · April 2012
- is an effective way to initiate recruitment of the supraspinatus muscle fibers
- This exercise can be progressed to "the full can acvivity", which is known th exhibit high supraspinatus muscle activity
AAROM ex
Deltoid reeducation
□ This deltoid muscle rehabilitation regimen, associated with pain medication, was effective in improving the function and pain in elderly patients with massive cuff tears, reverse total shoulder arthroplasty
Isometric & muscle recruitment
Back & periscapular exe
Started CKC exercise
□ started closed chain stability exercises
* improve neuromuscular control of the shoulder complex
□ Rhythmic stabilization(supine, quadruped)
* increase muscle activation and improve static stability of the shoulder complex
□ The exercise may be started at elevations of 60° or less and then moved up to 90° as tissue healing allows.
□ 3 weeks after surgery for glenoid labral repair or instability repair
□ 5 weeks after rotator cuff repairs
reference
Myers, Joseph B.shoulder muscle reflex latencies under various levels of muscle contraction.Clinical Orthopaedics & Related Research. 407:92-101, February 2003.
Frederick A. Matsen, III, Caroline Chebli and Steven Lippitt.Principles for the Evaluation and Management of Shoulder Instability.J Bone Joint Surg Am. 2006;88:647-659.
Morrey BF, An KN (1990)Biomechanics of the shoulder. In: Rockwood CR, Matsen FA (ed) The shoulder. Saunders, Philadelphia, pp 208–245Google Scholar.
Philip Mcclure, Lori A. Michener.Direct 3-dimensional measurement of scapular kinematics during dynamic movements in vivo.Published in Journal of shoulder and elbow surgery 2001
Parsons IM1, Apreleva M, Fu FH, Woo SL.The effect of rotator cuff tears on reaction forces at the glenohumeral joint.J Orthop Res. 2002 May;20(3):439-46.
MET
Young Jin Jo1, Young Kyun Kim.Consideration of Shoulder Injury Prevention and Rehabilitation Exercise for Overhead Sports Population.Asian J Kinesiol 2019; 21(2): 40-50 · DOI:https://doi.org/10.15758/ajk.2019.21.2.40
Ofer Levy, Hannan Mullett,The role of anterior deltoid reeducation in patients with massive irreparable degenerative rotator cuff tears.Medicine Published in Journal of shoulder and elbow surgery2005 DOI:10.1016/j.jse.2008.04.005
Olivier A. van der Meijden, MD1.Rehabilitation after arthroscopic rotator cuff repair: Current concepts review and evidence-based guidelines.International Journal of Sports Physical Therapy · April 2012
⇒ Avoided end range stretch (first 6 weeks), active exe
● Avoided pulley exe
● Avoided elevation from 30 to 60° (more 2 tendon injury, subscapularis injury)
Phase1 (1~4weeks)
▣ collagen deposition and growth factors increase, with a peak increase around 10 days after surgery
▣ repair should not be exposed to the excessive forces inposed by active motion
▣ Pressure at the end range (stretching) should be avoided for the first 6 weeks
▣ PROM is progressed with caution
□ Started periscapular activation
- isolated scapular depression, retraction performed and has shown to exhibit minimal posterior RC cuff activity
□ Approximately 20~30° of scapular plane
- preventing decreased blood flow in the supraspinatus
- increasing the subacromial space
PROM & Scpaular setting
reference
Myers, Joseph B.shoulder muscle reflex latencies under various levels of muscle contraction.Clinical Orthopaedics & Related Research. 407:92-101, February 2003.
Frederick A. Matsen, III, Caroline Chebli and Steven Lippitt.Principles for the Evaluation and Management of Shoulder Instability.J Bone Joint Surg Am. 2006;88:647-659.
Morrey BF, An KN (1990)Biomechanics of the shoulder. In: Rockwood CR, Matsen FA (ed) The shoulder. Saunders, Philadelphia, pp 208–245Google Scholar.
Philip Mcclure, Lori A. Michener.Direct 3-dimensional measurement of scapular kinematics during dynamic movements in vivo.Published in Journal of shoulder and elbow surgery 2001
Parsons IM1, Apreleva M, Fu FH, Woo SL.The effect of rotator cuff tears on reaction forces at the glenohumeral joint.J Orthop Res. 2002 May;20(3):439-46.
MET
Young Jin Jo1, Young Kyun Kim.Consideration of Shoulder Injury Prevention and Rehabilitation Exercise for Overhead Sports Population.Asian J Kinesiol 2019; 21(2): 40-50 · DOI:https://doi.org/10.15758/ajk.2019.21.2.40
Ofer Levy, Hannan Mullett,The role of anterior deltoid reeducation in patients with massive irreparable degenerative rotator cuff tears.Medicine Published in Journal of shoulder and elbow surgery2005 DOI:10.1016/j.jse.2008.04.005
Olivier A. van der Meijden, MD1.Rehabilitation after arthroscopic rotator cuff repair: Current concepts review and evidence-based guidelines.International Journal of Sports Physical Therapy · April 2012
합병증 보통 1.5% ~ 2.7%로 환자들의 어깨 움직임시 뻣뻣함 호소 > 치료시 신경써야한다.
재활가이드라인
회복 초기는 조직의 회복과 염증 통증감소 수술부위의 보호가 가장 중요.
수술 직후 4~6 주까지는 팔을 고정해주는 것이 중요하며 수술 후 어깨의 뻣뻣함 줄이기 위해 적절한 ROM운동이 필요하다.
회복과정은 3가지 단계로 구분
1 염증기 2 회복기 3재형성기
Operative treatment
Retear time rate
□ 22 patients with large or massive tears (>3cm)
- immobilization 4 week, strengthening 12 weeks
□ 66% retears, occurred within 3 months
□ 33% tetears, occurred after 6 months
□ No retears from 6 to 24 months
ROM gains
□ Type 1 : small tears (1cm, very good tissue quality)
- Full AROM 6~8 weeks
□ Type 2 : large tears ( <3~5cm, adequate tissue)
- Full AROM 8~12 weeks
□ Type 3 : large massive tears ( 3~5cm<, poor tissue, retracted tissue)
- Full AROM 12~16 weeks
Rotator cuff tensile strength
□ Ablilty to tolerate up to 100 N/mm of tensile strength
□ However, the tendons' endurance of compressive and shear forces is much less
□ Irritation and inflammation of the subacromial bursa which is rich in nerve fibers
Bursa
□ protection from shearing forces
□ contribute to the blood supply
□ healing of the rotator cuff particularly
□ preservation of the tissue
□ Bursectomy
- lead to rotator cuff tears or adhesions of the tendons of capsule
Tendon Healing Potential
□ Partial -thickness, small full thickness tears of the rotator cuff may heal spontaneously.
□ Most small tears will enlarge if not surgically repaired
Rotator cuff healing stage
염증기 > 증식기 > 재형성기
염증기
* Following surgical tendon-to-bone fixation
* Occurs first 7 days
* The release of histamine and bradykinin increases vascular permeability
* Inflammatory cells followed by platelets and fibroblasts migrate into the repair site
* Cellular proliferation and matrix deposition of this phase is thought to be regulated by several growth factors and initially yields primarily type 3 collagen.
증식기
* When next 2~3 weeks, begin to proliferate or repair
* This tissue replaces, which occurs 2 to 3 weeks after tendon ingury or repair
* Combine with capillary buds and nascent extracellular matrix to form granulation tissue.
재형성기
* During the following week(after 4weeks), this repair tissue grows stronger during the transition to the maturation phase.
* Scar tissue organizes through extracellular matrix turnover.
* The initial type 3 collagen deposition is slowly replaced by type 1
collagen, continuing until mature scar tissue is formed
* Remodeling repair tissue does not reach maximal tensile strength for a minimum of 12~16 weeks post repair, returned to maximal failure loads after only 26 weeks of healing.
Fisk factors of stiff shoulder after cuff repair
□ Calcific tendinitis
□ Adhesive capsulitis
□ PASTA type repair
□ Concomitant SLAP repair
□ Single tendon repair
Effect of immobilization
□ Postoperative immobilization can minimize the tension on rotator cuff repairs and may lead to improved collagen orientation and visco-elastic properties as compared to immediate postoperative exercise treatment
□ Immobilization of the shoulder for 4-6 weeks in a slightly abducted position may minimize tension and maximize vascularization of the repair
신장분사 치료
□ post-surgically to decrease pain, swelling, muscle spasm, and minimize the inflammatory response
□ authors recommend the use of a home cryotherapy device for 10-14 days after surgery
관절 가동술
□ 30도 abduction in the scapular plane
- anterior and posterior translational glides do not significantly alter stress on repaired supraspinatus tendons with the arm in resting position.
□ Especially, posterior translational glides have shown to significantly increase external rotation range of motion in patients with stiff shoulders.
□ Progressed ROM to 4-6 weeks after surgery
exercise
Joint play (posterior gliding)
Gird streching
Latissimus dorsi streching
Shoulder ER/IR
Shoulder retraction
Shoulder protraction
Scaption
eccentric contraction
reference
Myers, Joseph B.shoulder muscle reflex latencies under various levels of muscle contraction.Clinical Orthopaedics & Related Research. 407:92-101, February 2003.
Frederick A. Matsen, III, Caroline Chebli and Steven Lippitt. Principles for the Evaluation and Management of Shoulder Instability.J Bone Joint Surg Am. 2006;88:647-659.
Morrey BF, An KN (1990) Biomechanics of the shoulder. In: Rockwood CR, Matsen FA (ed) The shoulder. Saunders, Philadelphia, pp 208–245Google Scholar.
Philip Mcclure, Lori A. Michener. Direct 3-dimensional measurement of scapular kinematics during dynamic movements in vivo.Published in Journal of shoulder and elbow surgery 2001
Parsons IM1, Apreleva M, Fu FH, Woo SL. The effect of rotator cuff tears on reaction forces at the glenohumeral joint.J Orthop Res. 2002 May;20(3):439-46.
MET
Young Jin Jo1, Young Kyun Kim. Consideration of Shoulder Injury Prevention and Rehabilitation Exercise for Overhead Sports Population.Asian J Kinesiol 2019; 21(2): 40-50 · DOI: https://doi.org/10.15758/ajk.2019.21.2.40
Ofer Levy, Hannan Mullett, The role of anterior deltoid reeducation in patients with massive irreparable degenerative rotator cuff tears.Medicine Published in Journal of shoulder and elbow surgery2005 DOI:10.1016/j.jse.2008.04.005
Olivier A. van der Meijden, MD1. Rehabilitation after arthroscopic rotator cuff repair: Current concepts review and evidence-based guidelines.International Journal of Sports Physical Therapy · April 2012
During passive glenohumeral motion, limited evidence demonstrates that during 30~60° superior translation occurs
GH joint 운동형상학(kinematics)
First 30~60° at scapular plane
0.7~2.7mm anterior translation
60~90°
0~1.5mm posterior translation
90~120°
1~4.5mm posterior translation
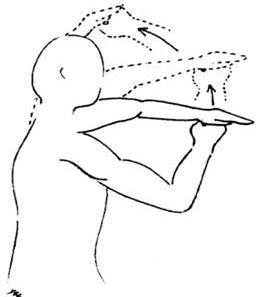
▶ Exernal rotation is important for clearance of the greater tuberosity during elevation
Effect of external rotation during elevation
▷increase humeral external rotation at scapular planethan sagittal and coronal plane.
▷Exernal rotation
its associated tissues as it passes under the coracoacromial arch
Effect of humeral ER
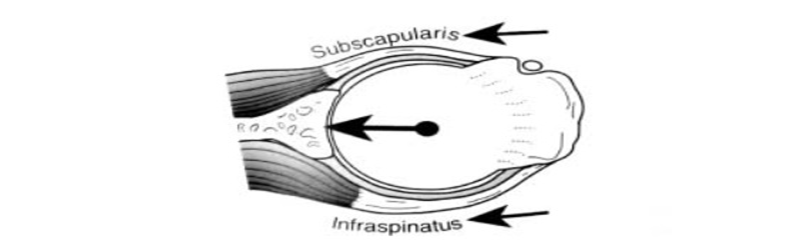
GH Joint Kinematics
● Subscapularis teres minor, infraspinatuscontribute to depression of the humeralin the glenoid cavity more than does the supraspinatus.And/or provides dynamic stability to the GH joint during deltoid activation.
Subacromial space
● Height of the subaromial space
▷ 1~1.5cm
● At 90 elevation(healthy)
▷ 4.1mm
● Shoulder impingement
▷ 1.4mm
⇒ 6mm Superior displacement of humeral head if rotator cuff tear space effect
출처
Myers, Joseph B.shoulder muscle reflex latencies under various levels of muscle contraction.Clinical Orthopaedics & Related Research. 407:92-101, February 2003.
Frederick A. Matsen, III, Caroline Chebli and Steven Lippitt. Principles for the Evaluation and Management of Shoulder Instability.J Bone Joint Surg Am. 2006;88:647-659.
Morrey BF, An KN (1990) Biomechanics of the shoulder. In: Rockwood CR, Matsen FA (ed) The shoulder. Saunders, Philadelphia, pp 208–245Google Scholar.
Philip Mcclure, Lori A. Michener. Direct 3-dimensional measurement of scapular kinematics during dynamic movements in vivo.Published in Journal of shoulder and elbow surgery 2001
Parsons IM1, Apreleva M, Fu FH, Woo SL. The effect of rotator cuff tears on reaction forces at the glenohumeral joint.J Orthop Res. 2002 May;20(3):439-46.
Young Jin Jo1, Young Kyun Kim. Consideration of Shoulder Injury Prevention and Rehabilitation Exercise for Overhead Sports Population.Asian J Kinesiol 2019; 21(2): 40-50 · DOI: https://doi.org/10.15758/ajk.2019.21.2.40
Ofer Levy, Hannan Mullett, The role of anterior deltoid reeducation in patients with massive irreparable degenerative rotator cuff tears.Medicine Published in Journal of shoulder and elbow surgery2005 DOI:10.1016/j.jse.2008.04.005
회전근은 어깨뼈에서 시작하여 위팔뼈 위쪽 부분에 붙는 가시위근, 가시아래근, 어깨밑근, 작은원근을 말한다. 가시위근은 팔을 벌리는 기능을 하고 가시아래근과 작은원근은 팔을 바깥으로 돌리는기능을 하며 어깨 밑근은 팔을 안쪽으로 돌리는 기능을 한다. 회전근은 팔을 움직이는 역할을 할 뿐 아니라 관절오목에 대하여 위팔뼈 머리의 안정성을 제공한다.
어깨관절은 그 자체만으로는 불안정하기 때문에 회전근은 어깨 관절의 안정성을 유지하는 데 매우 중요한 역할을 한다.
▷가시위근 : 어깨뼈의 가시위오목에서 시작하여 위팔뼈 큰결절의 윗 면에 붙는다. 어깨위신경의 지배를 받는다.
▷가시아래근 : 어깨뼈의 가시아래오목에서 시작하여 위팔뼈 큰결절의 중간면에 닿는다. 어깨위신경의 지배를 받는다.
▷작은원근 : 어깨뼈 가쪽모서리 중간에서 시작하여 위팔뼈 큰결절 아랫면에 닿는다. 겨드랑 신경의 지배를 받는다.
▷어깨밑근 : 어깨뼈의 밑오목에서 시작하여 위팔뼈 작은결절에 붙는다. 어깨밑신경의 지배를 받는다.